


A new 46-year-old male patient with a history of high myopia and lattice degeneration presented for a comprehensive exam during which I noted a blot hemorrhage and a cotton-wool spot in the superior area of his retina OD along the superior vascular arcade. His left eye appeared to be free of any type of retinopathy. The exam also revealed a large cup-to-disk ratio (.45/.45 OD, .55/.55 OS) in the context of a large optic nerve head size OU.
The patient reported an unremarkable systemic history, though divulged he had not seen a primary care physician (PCP) for an extended period. His only medications were OTC vitamins.
I explained to the patient that we found some bleeding in the back of his right eye, which is typically caused by high blood pressure or diabetes. When his blood pressure was measured in our office, it was 132/82. Accordingly, I stressed the need to schedule an appointment with a PCP for a complete physical and blood workup to help determine the cause of the hemorrhages.
Additionally, I explained I needed to see him in 4 months to ensure the retinal findings were not worsening, and to assess the health of his left eye.
Alas, he did not return until 2 years later.
Diagnosed and Progressing
At the patient’s second visit, he said he had a physical, as recommended, and was diagnosed as having type 2 diabetes, for which he was taking metformin.
Further, the patient reported that his blood sugar was pretty well controlled, and that his last HbA1c was 6.5. He denied any new ocular or visual complaints.
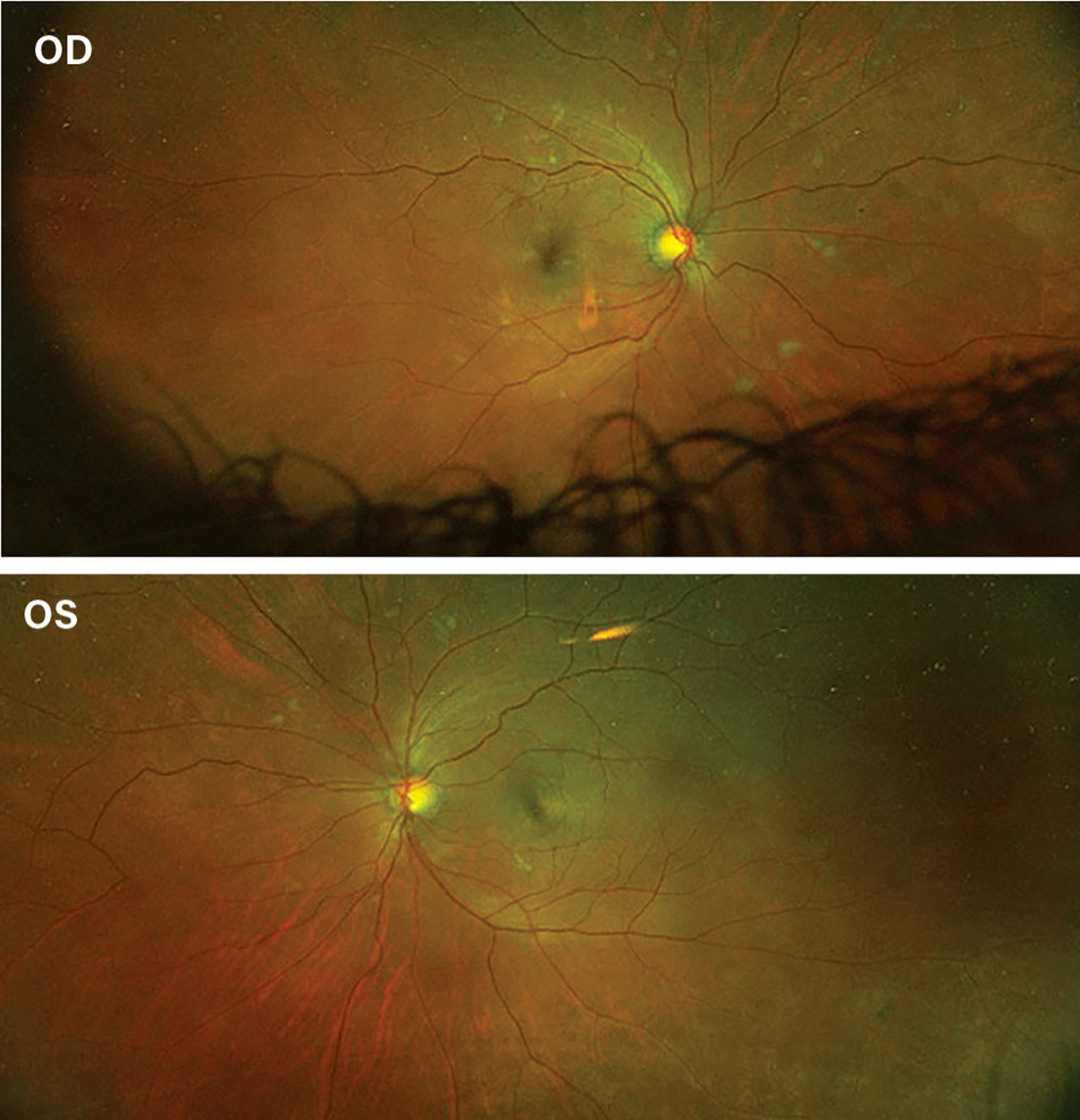
This comprehensive examination revealed increased cotton-wool spots OD and retinal hemorrhages OU.
As a result, I explained to the patient that his diabetic retinopathy (DR) had worsened and was now bilateral. I also emphasized to him the importance of working with his PCP and a nutritionist on a diet and exercise plan to help prevent further worsening of his condition.
Further, I provided thorough education on the risks of vision loss due to DR, and I asked the patient to return in 6 months for a follow-up exam.
This time, the patient returned 18 months later.
A Change in Treatment
During this visit, the patient explained that since his last eye exam he had stop-ped taking the metformin, due to its side effects. He divulged that this, in turn, caused his HbA1c to spike to 12.
The patient also said that his PCP convinced him to resume the treatment and prescribed a glucagon-like peptide-1 (GLP-1) agonist as a secondary treatment for his type 2 diabetes. This intervention led to significant weight loss and better control of his HbA1c. In fact, the patient reported that his last HbA1c test was a 6.He said he was proud of his weight loss, felt great, and believed that his vision was as good as ever. He stated, “The only reason I came in today is because I bet my wife that my diabetic bleeding has all gone away after starting [the injection], and I want you to tell her that I’m right.”
Unfortunately, the patient’s exam showed worsening DR OU. Specifically, I noted intraretinal hemorrhages in all 4 quadrants OU, as well as increased cotton-wool spots OU.
In addition, I noted hard exudates forming along his right macula, putting him at significant risk for macular edema.
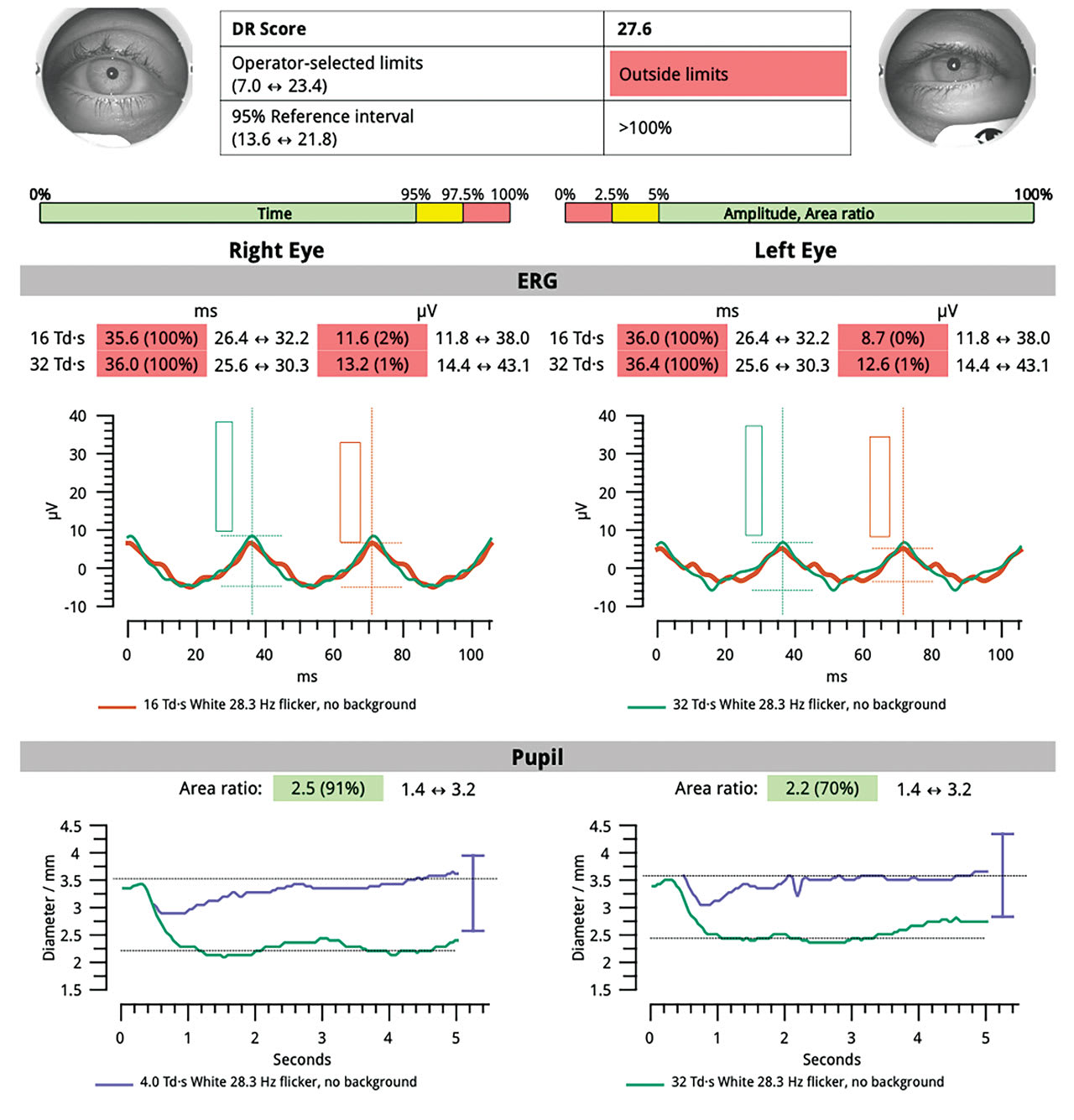
A handheld electroretinographer revealed severely delayed implicit time OU, along with severely reduced amplitude OU and a DR score of 27.6, which is outside of normal limits for this device. In fact, a score of 23.5 or higher indicates an 11-fold risk of requiring intervention within 3 years.1
At this time, I diagnosed the patient as having severe nonproliferative DR with possible macular edema OD.
A Research Connection?
Given the patient’s use of a GLP-1, it is worth noting that recent research implicates these medications as a factor for DR complications.2
Based on this research and the fact that GLP-1s are all the rage when it comes to both type 2 diabetes and weight loss, it makes sense for ODs to keep the effects of these interventions on retinal health on their radars. Ideally, this would involve screening patients before initiating treatment, as well as monitoring them closely while they are using a GLP-1 agonist.
Novo Nordisk A/S, a manufacturer of several GLP-1 agonists (semaglutide) is sponsoring the FOCUS trial to determine the long-term effects of semaglutide vs. placebo on diabetic eye disease, according to clinicaltrials.gov.
That Patient
After informing the patient that he lost his bet with his wife, I impressed upon him the importance of making an appointment with a retina specialist. This task was made easier when I explained the color-coded result from the ERG and his before and after fundus images. At press time, the patient saw a retina specialist, who found macular leakage, but not clinically significant macular edema. The patient will now be followed every 4 to 6 months. OM
References
1. Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N. Engl J Med. 2016;375:1834–44. doi: 10.1056/NEJMoa1607141.
2. Singh H, Natt NK, Nim DK. Association between glucagon-like peptide-1 agonists and risk of diabetic retinopathy: a disproportionality analysis using FDA adverse event reporting system data. Expert Rev Endocrinol Metab. 2025;20(2):147-152. doi:10.1080/17446651.2025.2459720).
