


With the proven track record of epi-off corneal crosslinking (CXL) in halting keratoconus (KCN) progression and the forthcoming availability of epi-on CXL, let’s discuss the specific steps optometrists should take in comanaging these patients.
Be a KCN Sleuth.
Because the early detection of KCN and progressive corneal ectasia are critical to CXL success, it’s imperative the OD have a corneal topographer and keratometer to make a timely referral. This referral should occur when the OD notes asymmetric corneal topography, steep K readings, Vogt’s striae, and/or loss of best-corrected spectacle vision.
Educate the Patient.
I have found that patients who receive complete and compassionate education from their OD are more likely to comply in a timely manner with referrals. When it comes to the CXL consult, I take a few minutes to define KCN, how it can progress (reducing best-corrected vision), how CXL works, and what the patient can expect both during and after the procedure. Also, I reassure the patient that they will not “go blind,” and that the need for a corneal transplant, while available, if necessary, remains very unlikely.
Whenever possible, I also have my administrator set up the CXL consultation before the patient leaves the office.
Choose Your Team.
Depending on a practice’s geographic area (ie, size and concentration of cornea and contact lens services), I recommend aligning with a minimum of 2 corneal specialists for CXL. This is to make convenient and high-quality care as geographically accessible as possible.
Further, I suggest meeting with them in person to ascertain personal and professional “compatibility.” As examples, are these specialists open to answering all the OD’s questions, providing their mobile phone numbers, and accommodating patients with timely and preferential appointments? Also, will they tell the optometrist where they perform CXL, their preferred protocol for contact lens (CL) removal prior to patient evaluation (if applicable), and when they typically return patients to the referring doctor?
Finally, the OD should meet with these specialists’ office managers/patient liaisons to provide their office hours and manager’s contact information to secure the comanagement relationship.
Provide Post-Procedure Care.
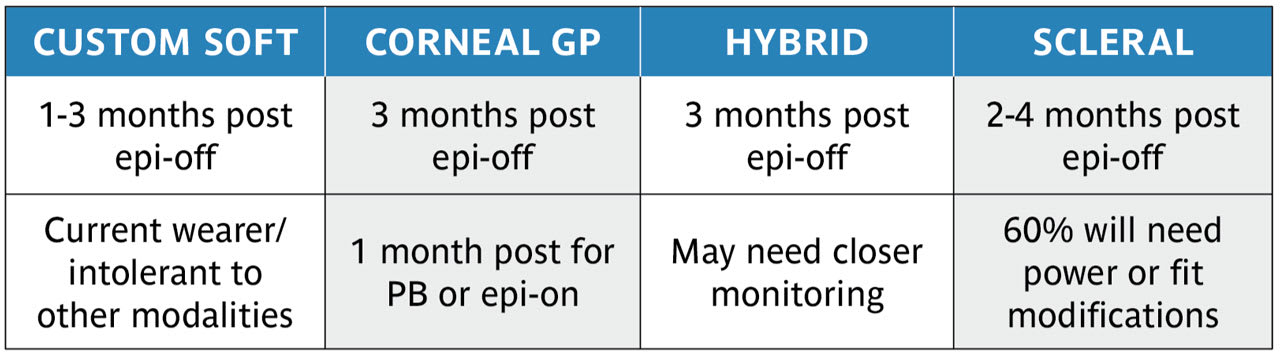
The optometrist should be ready to monitor postop medication use (ie, topical antibiotic and corticosteroids), and to initiate CL fitting or refitting (when necessary) after conducting a comprehensive corneal evaluation. The OD should communicate any concerning or unexpected events to the surgeon and discuss a management plan.
I obtain new “baseline” topo-graphical images, assess cornea health, and perform a manifest refraction. Upon confirming a healthy cornea (no staining or significant subepithelial haze), I initiate the CL evaluation. Once CL fitting is completed, I follow the patient every 3 months for the first 6 months and semi-annually going forward.
A Collaborative Relationship
With trusted corneal specialists has enabled me to render excellent patient care. OM
