


Currently, nearly 10 million (1 in 4) patients with diabetes have diabetic retinopathy (DR) in the United States, with 5% (1.84 million) having vision-threatening disease.1 Glucagon-like peptide-1 agonists (GLP-1), popular choices for the second-line treatment of type 2 diabetes and, most recently, obesity, are connected with DR. (See “GLP-1: An Overview,” p.11.) So, what’s the latest and its implications for practice? In this article, I explain.
The Latest
A recent study on GLP-1 agonists shows dulaglutide and semaglutide were strongly associated with worsening DR; liraglutide and tirzepatide had a weaker, though significant link; and lixisenatide had no major link with the blinding eye condition.2
The researchers arrived at these conclusions after analyzing data from the U.S. Food and Drug Administration Adverse Event Reporting System from Q4/2003 to Q2/2024 on the aforementioned GLP-1 agonists. Additionally, they used the key search term “diabetic retinopathy.”
The purpose of the study was to assess the link between these agonists and DR, as “Concerns have emerged regarding their potential link to diabetic retinopathy,” according to the study.
One theory for this association is the mechanism of action—the significant improvement of glycemic control—of GLP-1 agonists.3 This theory is based on previous studies linking accelerated improvement in glucose control from insulin with a temporary worsening of DR.4,5
It is also worth noting that past studies suggest GLP-1 agonists thwart retinal neurodegeneration.6,7 Thus, additional studies are needed to determine the effects of these interventions.
Incidentally, Novo Nordisk A/S, a GLP-1 agonist manufacturer, is sponsoring the FOCUS trial to assess the long-term effects of its GLP-1 agonist vs. placebo on diabetic eye disease, shows clinicaltrials.gov.
The study, which started in May 2019, has enrolled 1,500 patients who have type 2 diabetes and have been randomized into the GLP-1 agonist or placebo treatment arm. The trial’s estimated completion date is November 2027.
Implications for Practice
Due to the established connection between GLP-1 agonists and DR, optometrists should err on the side of caution and be in contact with primary care physicians on whether GLP-1/gastric inhibitory polypeptide (GIP) agonists should be prescribed in patients who have existing DR. Additionally, it has been recommended to shorten follow-up periods for patients using a GLP-1 agonist for more frequent screenings (6 to 12 weeks), especially if DR is present or the patient reports vision loss since their last visit.8
The baseline and follow-up eye exams can include the following assistive technologies:
• Artificial intelligence technologies. EyeScreen (Eyenuk, Inc.) iCare ILLUME (Centervue), the LumineticsCore (Digital Diagnostics), and iPrevent DR (iHealthScreen) are available to aid in both the screening and monitoring of DR in the United States.
• B-Scan ultrasonography. This tool enables the identification of a vitreous hemorrhage or media opacities.
• Fundus photography. Whether using standard retinal photography (30° of view) or ultra-widefield imaging (a larger field of view), fundus photography aids the OD in identifying peripheral lesions in the posterior pole.
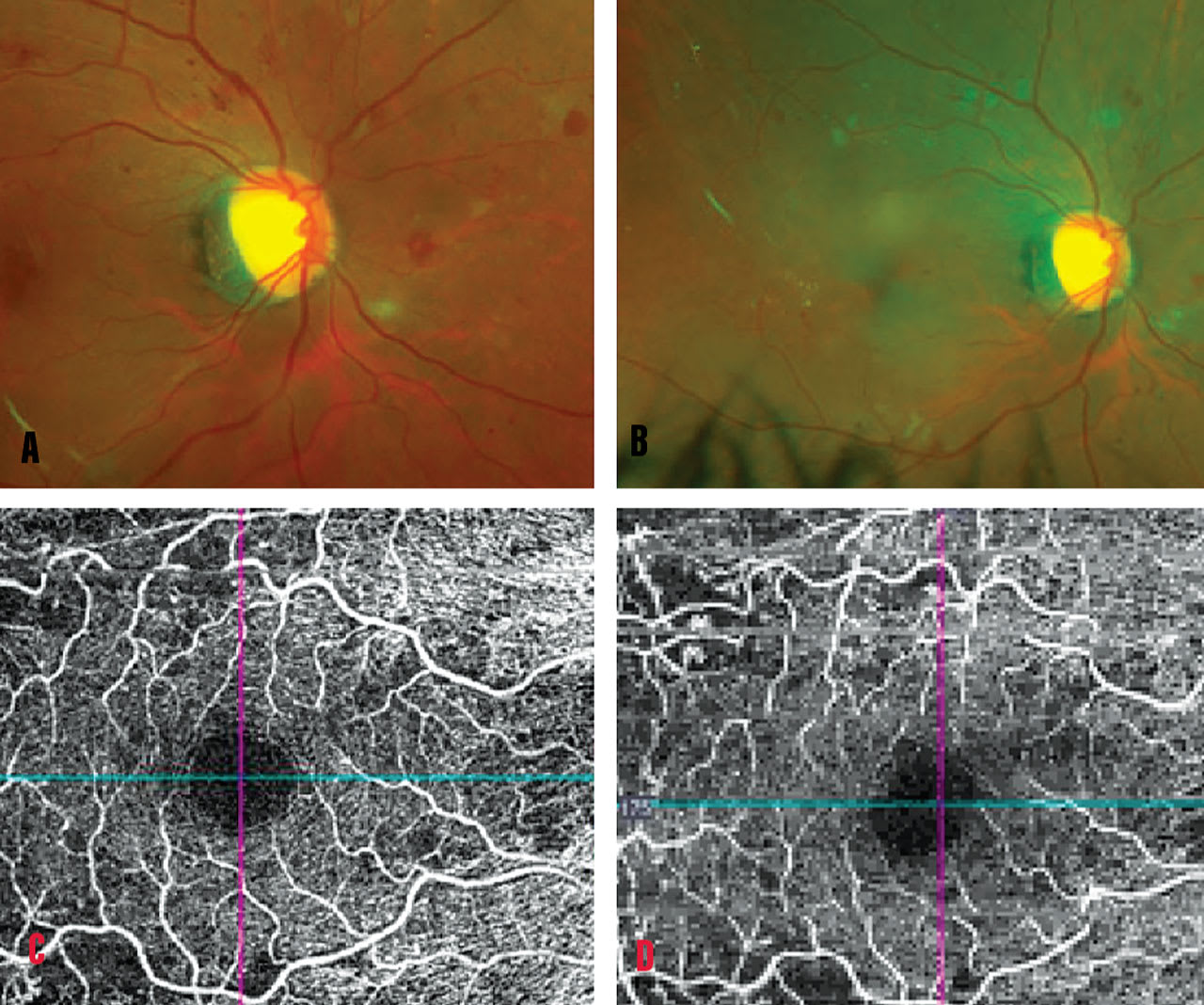
• Optical coherence tomography angiography (OCT-A). This technology helps the OD identify subclinical microaneurysms at the deep capillary plexus, dilations of the vessels, intraretinal microvascular abnormalities, capillary non-perfusion, vascular loops, vascular tortuosity, and neovascularization. Additionally, OCT-A can reveal diabetic macular ischemia (which appears clinically as areas of capillary nonperfusion), enlargement of the foveal avascular zone, and choriocapillary flow impairment. Widefield OCT is also available that can allow for the detection of peripheral retinal vascular abnormalities.
• Spectral-domain OCT. This helps the optometrist identify center-involving diabetic macular edema (DME). DME appears as loss of foveal contour, and cystoid macular edema, as well as neurosensory detachment in the fovea’s center. Further, there is an increased central macular thickening measurement.
• Widefield fluorescein angiography and indocyanine green (IGC) angiography. These technologies aid the OD in identifying peripheral capillary network nonperfusion.
Something to keep in mind: Technologies are also available that assist the OD in spotting compromised early visual function, such as decreased color and contrast sensitivity, and abnormal electrophysiology of the retina due to abnormal vision. (See “Case Study: Electroretinography in Diabetic Retinopathy,” also in this issue.)
Further, because carotenoids can curb DR development, the optometrist should consider using a macular pigment optical density device.
In addition to monitoring for progressive DR with the assistive technologies discussed, prophylactic treatment with anti-VEGF injections should be considered to reduce DR progression.9
In some cases of worsening DR and persistent DME after 3 to 6 injections, a retina specialist
may elect to switch to newer extended treatment anti-VEGF or combination anti-VEGF/Angiopoietin-2 (Ang-2) inhibitor agents, a laser, steroids, or a port delivery system. (See “Diabetic Retinopathy Management: Preparing Patients,” online.)
Taking Action
As the primary eyecare providers, ODs must be aware of any possible links among systemic drugs and adverse ocular events. (See “Non-Arteritic Anterior Ischemic Optic Neuropathy and GLP-1 Agonists,” below.) With the recent popularity of this second-line treatment for type 2 diabetes and obesity and the latest research, we can play a crucial role in identifying progressive disease.
GLP-1: An Overview
Glucagon-like peptide-1 (GLP-1) agonists act by stimulating insulin secretion in hyperglycemic states, suppressing glucagon secretion in hyperglycemic or euglycemic states, delaying gastric emptying, decreasing appetite, and reducing body weight.10
They can be administered via subcutaneous injection or orally. The subcutaneous injections available in the United States are dulaglutide (Trulicity, Eli Lilly, for type 2 diabetes), liraglutide (Victoza, Novo Nordisk, for type 2 diabetes), semaglutide (Ozempic, Novo Nordisk, for type 2 diabetes and Wegovy, for weight loss), tirzepatide (Mounjaro, Eli Lilly, for type 2 diabetes), and Zepbound (Eli Lilly, for weight loss). The oral version available in the United States is semaglutide (Rybelsus, Novo Nordisk), which is a tablet version of semaglutide for type 2 diabetes.
Non-Arteritic Anterior Ischemic Optic Neuropathy and GLP-1 Agonists
There is growing concern regarding the increased risk of Non-arteritic anterior ischemic optic neuropathy (NAION) and glucagon-like peptide-1 (GLP-1) agonists.11
NAION can cause optic neuropathy. A recent study published in JAMA Ophthalmology reveals an elevated risk of NAION for those exposed to semaglutide.12
Patients using this GLP-1 agonist should be counseled to see their eyecare provider immediately if they experience sudden loss of vision.
References
1. Lundeen EA, Burke-Conte Z, Rein DB, et al. Prevalence of diabetic retinopathy in the US in 2021. JAMA Ophthalmol. 2023;141(8):747-754. doi: 10.1001/jamaophthalmol.2023.2289.
2. Singh H, Natt NK, Nim DK. Association between glucagon-like peptide-1 agonists and risk of diabetic retinopathy: a disproportionality analysis using FDA adverse event reporting system data. Expert Rev Endocrinol Metab. 2025;20(2):147-152. doi:10.1080/17446651.2025.2459720
3. Joo JH, Sharma N, Shaia J, et al. The Effect of Glucagon-Like Peptide-1 Receptor Agonists on Diabetic Retinopathy at a Tertiary Care Center. Ophthalmol Sci. 2024;4(6):100547. Published 2024 May 6. doi:10.1016/j.xops.2024.100547.
4. Early worsening of diabetic retinopathy in the Diabetes Control and Complications Trial [published correction appears in Arch Ophthalmol 1998 Nov;116(11):1469]. Arch Ophthalmol. 1998;116(7):874-886. doi:10.1001/archopht.116.7.874.
5. Akil H, Burgess J, Nevitt S, Harding SP, Alam U, Burgess P. Early Worsening of Retinopathy in Type 1 and Type 2 Diabetes After Rapid Improvement in Glycaemic Control: A Systematic Review. Diabetes Ther. 2022;13(1):1-23. doi:10.1007/s13300-021-01190-z.
6. C. Hernández, P. Bogdanov, L. Corraliza, et al. Topical administration of GLP-1 receptor agonists prevents retinal neurodegeneration in experimental diabetes. Diabetes, 65 (2015), pp. 172-187 C. Hölscher. Potential role of glucagon-like peptide-1 (GLP-1) in neuroprotection CNS Drugs, 26 (2012), pp. 871-882.
7. Pang B, Zhou H, Kuang H. The potential benefits of glucagon-like peptide-1 receptor agonists for diabetic retinopathy. Peptides. 2018;100:123-126. doi:10.1016/j.peptides.2017.08.003.
8. American Academy of Ophthalmology. Update on Semaglutide Risks. Clinical Update. America Academy of Ophthalmology Eyenet journal. 2021. Accessed March 15, 2025. https://www.aao.org/eyenet/article/update-on-semaglutide-risks
9. Rajagopal R, McGill JB. NOVEL AGENTS IN THE MANAGEMENT OF DIABETES AND RISK OF WORSENING DIABETIC RETINOPATHY. Retina. 2024;44(11):1851-1859. doi:10.1097/IAE.0000000000004252.
10. Müller TD, Finan B, Bloom SR, et al. Glucagon-like peptide 1 (GLP-1). Mol Metab. 2019;30:72-130. doi:10.1016/j.molmet.2019.09.010
11. Cai CX, Hribar M, Baxter S, et al. Semaglutide and Nonarteritic Anterior Ischemic Optic Neuropathy. JAMA Ophthalmol. 2025;143(4):304-314. doi:10.1001/jamaophthalmol.2024.6555.
12. Rizzo JF 3rd, Hathaway JT. Semaglutide and Risk of NAION-Additional Insights. JAMA Ophthalmol. 2025;143(4):315-316. doi:10.1001/jamaophthalmol.2025.0005.
