


Case Presentation
A 60-year-old female patient presented for routine evaluation as a narrow angle glaucoma suspect. She had been diagnosed with anatomically narrow angles 6 years earlier and was placed on nightly topical hypotensive therapy. On medication, her intraocular pressures remained stable with no evidence of progressive optic neuropathy or visual field loss.
Despite stability, the patient reported worsening dry eye symptoms, redness, and irritation, which she attributed to her evening drop use. She asked whether alternative treatment options were available.
Treatment Considerations
In cases of anatomically narrow angles without symptoms of intermittent angle closure or glaucomatous damage, management should be individualized. Options include:
Alternative Topical Therapy. For stable patients, switching to a different hypotensive agent may improve tolerability. However, this approach often requires trial and error while monitoring for maintained pressure control.
Laser Peripheral Iridotomy. For patients not ready for cataract surgery, laser peripheral iridotomy (LPI) provides a prophylactic outflow pathway to reduce the risk of acute angle closure attacks and chronic intermittent angle closure symptoms.
Cataract Extraction. If the crystalline lens demonstrates visually significant opacity or contributes substantially to anterior chamber crowding, lens extraction can be a definitive solution by deepening the anterior chamber.
Observation. Careful monitoring without intervention may be appropriate in select patients, provided they are well counseled and adhere to regular surveillance.
Imaging-Guided Decision Making
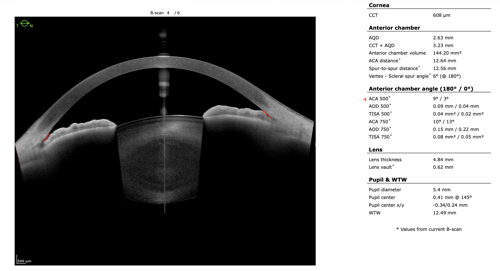
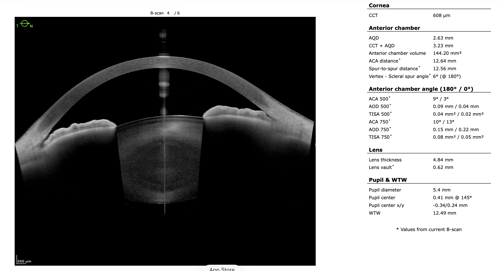
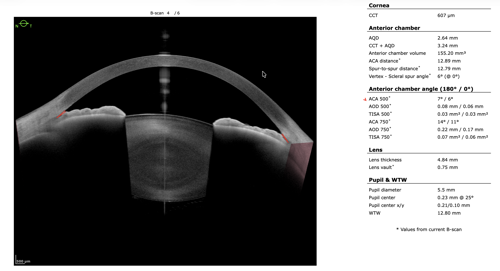
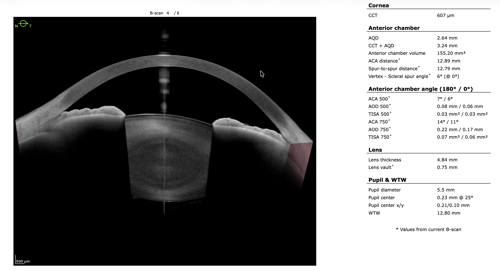
To refine surgical candidacy, anterior segment imaging was performed using the Heidelberg ANTERION SS-OCT. High-resolution imaging clearly demonstrated the following:
- A visually clear crystalline lens, not meeting criteria for cataract extraction
- Markedly narrow angles at iris insertion
- Angle measurements in the single-digit degrees
These findings supported LPI as the most appropriate intervention.
After discussing continued medical therapy, medication adjustment, observation, and LPI, the patient elected to proceed with LPI. The procedure was well tolerated. At follow-up, intraocular pressure, optic nerve appearance, and visual field testing remained stable.
Clinical Takeaway
Advanced anterior segment imaging allows efficient, objective evaluation of angle anatomy and surgical candidacy. In this case, imaging supported a definitive intervention that spared the patient years of chronic drop burden and improved her ocular surface discomfort, all while maintaining stable glaucoma surveillance outcomes.

This content is sponsored by Heidelberg