


For nearly any type of corneal pathology, scleral lenses are highly effective at managing vision needs as the lens vaults completely over corneal irregularities. However, lens considerations become more complicated when a patient presents with both corneal and scleral abnormality. Whether due to pathology or surgical alteration, a highly irregular sclera can cause many patient-doctor teams to encounter repeated lens fitting failures. Filtering blebs are a common example for which achieving a successful fit over an irregular landing zone is dictated not only by patient comfort and vision but also by respecting the integrity of their bleb function.
A 64-year-old female patient presented for scleral lens evaluation of her left eye (OS) with a history of post-LASIK ectasia and primary open-angle glaucoma. She had undergone glaucoma surgery resulting in a large superior-nasal filtering bleb. While she functioned well with a scleral lens in her right eye, multiple prior attempts in the left eye had failed due to persistent discomfort.
Examination revealed advanced corneal irregularity and a prominent irregular bleb. A scleral lens was indicated given her intolerance to corneal gas permeable (GP) lenses. However, the presence of the bleb complicated the fitting process. It was clear that the patient would need an impression-based scleral lens due to the level of regional customization needed, but this impression had to be taken over a soft, movable bleb. Thus, the integrity of the bleb filtration beneath the lens was uncertain. While slit lamp evaluation provided a surface-level assessment, it offered limited insight into how the lens affected intra- and sub-conjunctival space beneath.
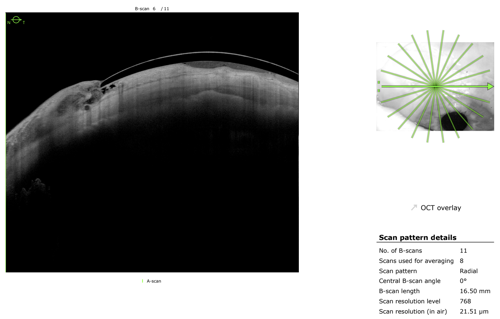
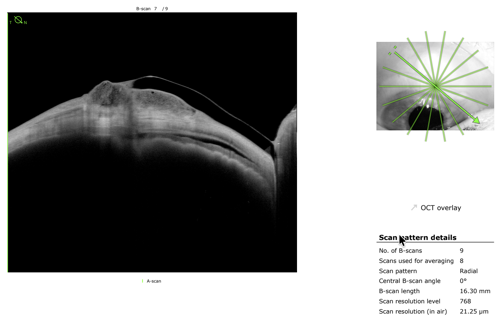
At the slit lamp, the lens appeared acceptable, yet the patient continued to report discomfort. As such, high-resolution anterior segment imaging with swept-source OCT was ordered to provide additional insight. Cross-sectional imaging revealed subtle but clinically significant compression of the bleb by the lens landing zone—findings not apparent at the slit lamp. Guided by this information, targeted modifications were made to redistribute pressure and improve alignment over the elevated tissue.
After 2 iterations, an optimal fit was achieved with improved comfort and stable vision. Most importantly, the bleb remained uncompromised.
This case underscores an important principle: In complex anterior segment cases, clinical appearance alone may not reflect true physiologic interaction. The level of detail and penetration of swept-source OCT allows clinicians to visualize lens-tissue relationships with a level of precision that enhances both safety and success.
In this case, seeing beneath the surface made the difference between repeated failure and meaningful clinical success.

This content is sponsored by Heidelberg